Every clinic operator in the UAE eventually runs into the same operational fork: a patient walks in and pays on the spot, and twenty minutes later another patient walks in whose entire visit depends on an insurer’s approval, network tier, and contracted rate. Same clinic, same chair, two completely different financial paths.
This isn’t a Dubai-specific reality. It plays out the same way in Abu Dhabi, Sharjah, and the Northern Emirates — except each jurisdiction runs its own regulator, its own health information exchange, and its own rules for what you can charge and how you must bill it. A clinic with locations in more than one emirate, or one simply trying to get pricing and billing right in a single emirate, needs to understand these differences at a granular level — not just at the level of “cash is simple, insurance is complex.”
This piece goes past that general framing and into the mechanics: how to actually build a defensible cash price list, how insurance pricing really gets set, what changes in your billing workflow the moment a patient is tagged as “insured” instead of “self-pay,” and how to keep your revenue mix from quietly becoming a liability.
The UAE isn’t one market — it’s four regulatory environments
Pricing and billing rules for healthcare in the UAE are set at the emirate level, not federally. A clinic that treats Abu Dhabi patients the same way it treats Dubai patients — administratively speaking — will eventually run into friction, usually in the form of a rejected claim or a data submission error.
| Emirate | Regulator | Health information exchange | Claims pathway |
| Dubai | DHA | NABIDH | eClaimLink / DHPO |
| Abu Dhabi | DoH | Malaffi | Riayati-linked claims processing |
| Sharjah | SHA (formerly under MOHAP) | Riayati / federal exchange | Transitioning under SHA licensing as of the August 2026 deadline |
| Northern Emirates | MOHAP | Riayati | MOHAP-governed submission rules |
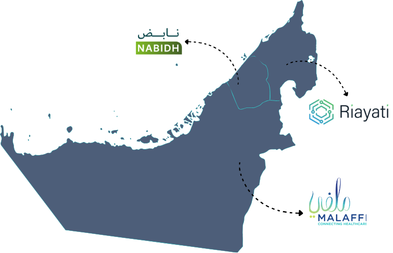
The practical impact of this fragmentation shows up in three places: which coding standards your billing team must apply, which portal a claim gets submitted through, and how quickly you can expect payment. A clinic operating across emirates should never assume a single pricing and billing playbook transfers cleanly from one jurisdiction to the next.
Pricing: two very different starting points
Cash pricing and insurance pricing aren’t two versions of the same number. They come from entirely different logic, and treating them as if they should always be closely tied together is where many clinics get into trouble.
Building a cash price list that holds up
A cash price should never be a guess or a round number picked because it “feels right.” A defensible cash price list is typically built from four inputs:
- True cost per service — clinical time, consumables, equipment depreciation, and a share of fixed overhead.
- Local market positioning — what comparable clinics in your area and tier are charging for the same procedure.
- Package logic — bundling consultation + diagnostic + first treatment into a single cash price is common in UAE clinics and tends to perform well with self-pay patients who want price certainty upfront.
- Margin targets by service line — some services (elective, aesthetic) can carry higher margins; others (routine checkups) are often priced closer to cost to drive volume and retention.

Where clinics lose discipline is in ad-hoc discounting — a front desk staff member shaving 10% off because a patient asked, with no record of why. Over a year, untracked discounting can quietly erode margin far more than any single pricing decision.
Insurance pricing: you’re not setting a price, you’re accepting one
This is the part that trips up clinics that are used to cash-only pricing logic. With insurance patients, your clinic isn’t pricing the service — it’s billing against a contracted fee schedule that was negotiated (or accepted) when you joined a payer’s network. Your only real levers are:
- Which networks and payers you choose to contract with in the first place
- How accurately you code the service you actually delivered
- Whether you bill every eligible component of a visit, or leave billable items on the table
This means insurance profitability is won or lost in billing accuracy, not in pricing strategy. A clinic can have excellent contracted rates and still underperform financially if coding is inconsistent or if staff default to the easiest code rather than the correct one.

A pricing detail most clinics overlook: VAT treatment
Cash and insurance transactions are often documented differently for VAT purposes. A walk-in cash patient can typically be issued a simplified tax invoice, while insurance billing — especially when the payer, not the patient, is the recipient of the service for VAT purposes — may require a full tax invoice carrying both parties’ TRNs. Getting this wrong doesn’t just create an accounting headache; it can affect your ability to claim input tax credit and creates exposure during an FTA audit. This is a detail worth confirming with your accountant per payer relationship, not assuming applies uniformly.
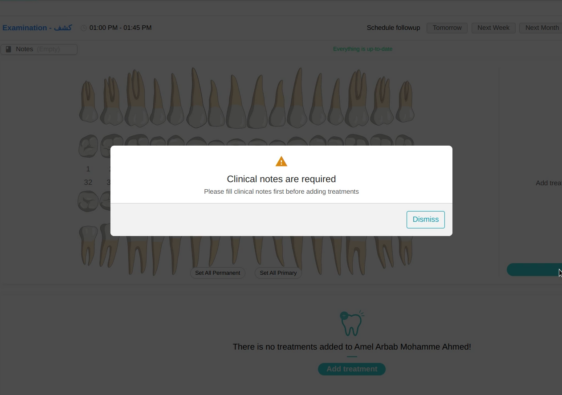
Billing: where the two workflows actually diverge
Pricing sets the number. Billing is what actually gets that number collected — and this is where cash and insurance patients require genuinely different operational tracks from the moment they’re registered.
Tagging the patient correctly, from the first touchpoint
The single biggest source of billing errors in mixed-payer clinics is a patient being registered incorrectly at the front desk — insurance details entered late, wrong network selected, or a patient assumed to be self-pay when they actually have partial coverage. Everything downstream depends on this being right the first time: which fee schedule applies, which invoice template gets generated, and whether a pre-approval step is even triggered.
Two different invoicing paths
Once a patient is correctly tagged, the invoicing logic splits:
- Cash patients receive a point-of-sale invoice at the time of service, generally paid in full before or immediately after treatment. Simple, but it needs to reflect the correct VAT treatment and an accurate service description — not a generic line item.
- Insurance patients generate two things: a claim submitted to the payer for the covered portion, and a separate patient-responsibility invoice for anything not covered — co-payment, deductible, or services excluded from the policy. Many clinics under-collect here simply because the patient-responsibility portion isn’t calculated and requested at the point of care, and instead becomes a chase-down after the visit.
Reconciliation looks nothing alike either
Cash reconciliation is a same-day exercise — matching till receipts to appointments. Insurance reconciliation is ongoing: matching remittance advices against submitted claims, identifying partial payments, tracking denials, and resubmitting corrected claims within payer deadlines. A clinic that applies a cash-style “close it out today” mentality to insurance billing will always have an ageing, unreconciled claims backlog.
Common billing mistake in mixed-payer clinics
Treating the patient-responsibility invoice as an afterthought. When co-pays and non-covered charges aren’t communicated and collected at the time of service, clinics end up trying to collect small amounts from patients weeks later — a process that costs more in staff time than the amount actually recovered, and damages the patient relationship in the process.
Balancing the two: it’s a portfolio decision, not just an operational one
Beyond getting pricing and billing right individually, clinic owners need to think about their cash-to-insurance mix the way a business thinks about revenue diversification.
Know your actual mix — not your assumed one
Many clinic owners have a rough sense of their patient mix but haven’t actually measured it by revenue, not just patient count. A clinic might see 60% of patients paying cash but generating only 35% of revenue, because average insurance claim values are higher per visit. Decisions about staffing, marketing spend, and even chair scheduling should be based on the revenue-weighted mix, not the headcount mix.
The risk of leaning too far either way
Over-reliance on one payer type creates two different failure modes:
- Too insurance-heavy: cash flow becomes hostage to payer processing times, and a single major payer tightening its policies or delaying payments can create a liquidity crunch.
- Too cash-heavy: revenue is more volatile month to month, more sensitive to local competition and discounting pressure, and harder to forecast.
Most stable UAE clinics deliberately manage toward a target mix rather than letting it emerge by accident, and revisit that target as their local competitive landscape and payer contracts shift.
Cash flow forecasting has to account for the lag
A clinic forecasting revenue the same way for both patient types will consistently misjudge its cash position. Cash revenue is realized the day it’s earned. Insurance revenue needs to be forecast with a lag built in — typically weeks, sometimes longer if claims are contested — and a portion should be discounted for expected denials or partial payments. Clinics that forecast both streams identically tend to be repeatedly surprised by cash shortfalls even when “revenue” on paper looks healthy.

Give your front desk team a decision tree, not just training
Training staff once on “how to handle insurance patients” isn’t enough when the actual daily decisions are nuanced — which invoice template to use, whether a pre-approval is required for a specific procedure, how to explain a co-payment amount to a patient who wasn’t expecting it. Clinics that document this as a simple, visual decision tree at the front desk see far fewer downstream billing errors than those relying purely on staff memory or verbal training.
Metrics that tell you whether the balance is actually working
A handful of numbers, tracked monthly, will tell you more about your cash-insurance balance than any qualitative sense of “things feel busy”:
- Revenue mix by payer type (not just patient count by payer type)
- Average days to payment, cash vs. insurance
- Claim denial and resubmission rate
- Patient-responsibility collection rate at point of care vs. collected later
- Discount rate on cash transactions, tracked against a defined policy
If any of these numbers are being estimated rather than pulled from your system, that’s usually the first sign the balance between cash and insurance isn’t actually being managed — it’s being tolerated.
How Balsam Medico supports this in practice
A lot of the friction described above comes down to systems that don’t distinguish clearly enough between how cash and insurance patients need to be handled. Balsam Medico is built with that distinction in mind:
- Patient-type tagging at registration that automatically routes the correct fee schedule, invoice template, and VAT treatment from the first touchpoint.
- Separate invoicing logic for point-of-sale cash receipts and patient-responsibility invoices, so co-pays and non-covered charges are calculated and presented at the time of service.
- Revenue mix reporting that shows payer split by revenue, not just by patient volume, so decisions are based on real numbers.
- Discount tracking tied to policy, so cash pricing stays consistent, and every exception is logged and explainable.
- Multi-emirate configuration for clinics operating under more than one regulator, keeping coding and submission rules aligned with the relevant authority.
The goal isn’t to make cash and insurance patients look the same in your system — it’s to give each the workflow it actually needs, without your team having to remember the differences manually every time.
Closing thought
Cash and insurance patients will always require different pricing logic and different billing mechanics — that’s not a problem to be solved away, it’s simply the operating reality of a clinic in the UAE. The clinics that do well aren’t the ones that pick a favourite between the two. They’re the ones that price each correctly, bill each accurately, and treat the mix between them as something to measure and manage deliberately, rather than something that just happens.
Connect with Us
Ready to embark on this exciting journey? Contact us today:
📍 Dubai, United Arab Emirates – Tel: +971 56 640 9602
📍 Khartoum, Sudan – Tel: +249 91 273 1048
Explore Balsam Medico and discover a world of efficient clinic management at www.balsammedico.com. Together, let’s reduce fines, elevate efficiency, and embrace a new era of dental healthcare.
One last thing..
PS: We built Balsam Medico to be the best software for clinics in UAE and the middle east. It is powerful, flexible, and most importantly, very easy to use.
If you have two minutes, see how it works.
This is the main landing page to learn more.