If you manage billing for a DHA-licensed clinic, you’ve almost certainly typed the letters “DHPO” into a support ticket, a claim rejection report, or a frustrated email to your EMR vendor. Yet the term itself remains one of the most misunderstood pieces of Dubai’s healthcare infrastructure — often used interchangeably with eClaimLink, sometimes confused with NABIDH, and rarely explained in plain terms to the people who actually have to work with it every day.
This guide breaks down what DHPO actually is, how it fits into Dubai’s claims ecosystem, and the specific compliance obligations your clinic needs to meet to avoid rejected claims, delayed reimbursements, and inspection flags.
What Is DHPO?
DHPO stands for the Dubai Health Post Office. It’s the electronic messaging and transaction gateway operated by the Dubai Health Authority (DHA) that carries insurance claims, pre-authorization requests, eligibility checks, and related financial transactions between healthcare providers and payers (insurance companies and third-party administrators).
Think of it less as a single website and more as a postal sorting system for healthcare finance. When your clinic submits a claim, DHPO is the pipe it travels through on its way to the insurer — validating the format, routing it to the correct payer, and returning acknowledgements, errors, or adjudication results back to you.
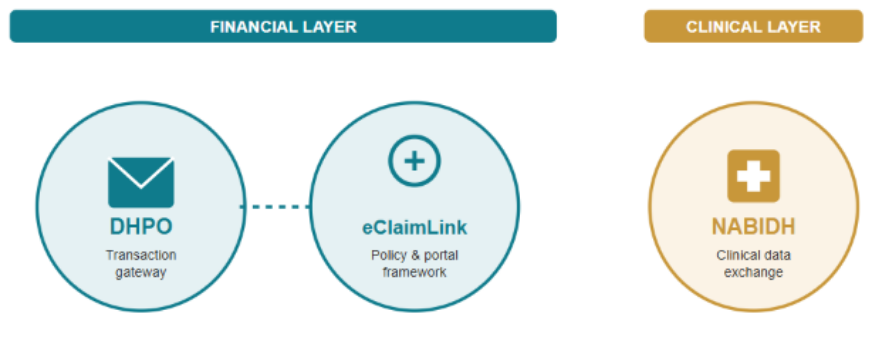
DHPO is the transaction backbone underneath eClaimLink, DHA’s broader claims management program. eClaimLink is the policy framework, business rules, and the portal interface providers log into; DHPO is the underlying system actually moving the data. In everyday clinic conversation, the two terms get used almost interchangeably, but technically eClaimLink is the initiative and DHPO is the engine.
DHPO vs. eClaimLink vs. NABIDH: Don’t Mix These Up
This is where most confusion happens, because all three acronyms come from the DHA and all three appear in the same compliance conversations. They do very different jobs, and mixing them up is one of the more common mistakes we see clinic teams make when preparing for an inspection.
| System | What it does | What it moves |
| DHPO | Claims transaction gateway between providers and payers | Financial data — claims, pre-auth requests, eligibility, remittances |
| eClaimLink | The overarching DHA program and portal for claims policy and submission | Business rules, provider/payer registration, portal access |
| NABIDH | Clinical health information exchange for Dubai | Patient medical records — history, diagnoses, prescriptions, lab results |
The distinction that matters most for compliance: DHPO and eClaimLink handle money, NABIDH handles medical records. A clinic can have a perfectly healthy DHPO integration and still be non-compliant on NABIDH, or vice versa. DHA inspectors check both, but they’re evaluating entirely separate obligations.
A Bit of Background: Why DHPO Exists
DHPO didn’t appear in isolation — it grew out of Dubai’s push toward mandatory health insurance and the DHA’s broader effort to standardize how claims move through the system. Before electronic claims infrastructure existed, providers and payers exchanged paper claims and faxed authorizations, a process that was slow, inconsistent, and difficult to audit. As Dubai’s insured population expanded following Law No. 11 of 2013, the volume of claims moving through the system made that old model unworkable.
DHA built eClaimLink as the governing framework for this shift, with DHPO as the transaction layer carrying the actual data. Over time, DHPO’s scope grew beyond simple claims to include member registration, eligibility verification, pre-authorization, and eventually ePrescription transactions — reflecting DHA’s broader intent to bring the entire financial and prescribing cycle onto a single, auditable electronic backbone. Understanding this history is useful context: DHPO isn’t a static system that was built once and left alone. It has evolved through multiple circulars and rule updates since its introduction, and clinics that treat their DHPO setup as a “set it and forget it” configuration are more likely to fall behind as those rules change.
Why DHPO Matters for Your Clinic
Health insurance has been mandatory for Dubai residents since Dubai Law No. 11 of 2013. In practical terms, this means the overwhelming majority of patients walking into a private clinic in Dubai are carrying employer-sponsored or individual insurance — not paying cash. Any DHA-licensed facility that treats these patients is expected to maintain an active DHPO integration to submit their claims electronically.
A clinic operating exclusively on a cash-pay basis, with zero insured patients, is technically outside this requirement. In practice, this is rare across Dubai’s private healthcare market given how deeply insurance penetration runs, so for most clinics, dental practices, and polyclinics, a working DHPO connection isn’t optional infrastructure — it’s a baseline requirement for doing business.
Clinics without a live DHPO integration are forced to fall back on manual entry through individual insurer portals, one payer at a time. This dramatically increases coding errors, slows down reimbursement, and creates exactly the kind of inconsistent billing trail that draws attention during a DHA facility inspection. What looks like a back-office inconvenience quickly becomes a compliance exposure.
How a Claim Actually Moves Through DHPO
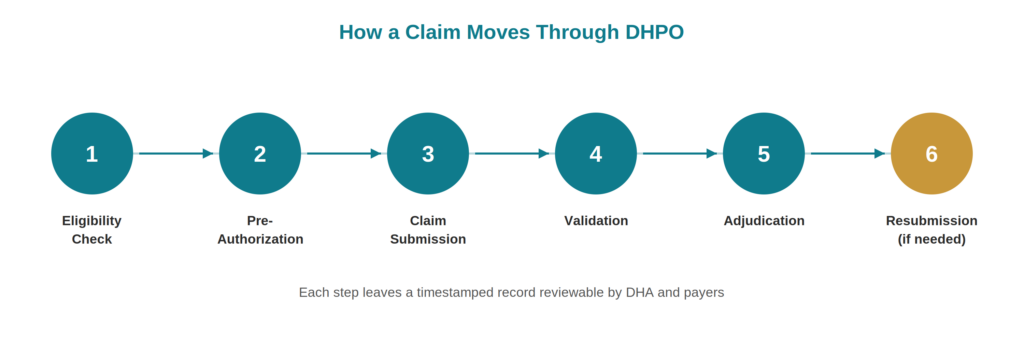
Understanding the mechanics helps explain where things typically go wrong. A standard eClaim cycle through DHPO looks roughly like this:
- Eligibility check: The clinic verifies the patient’s insurance coverage and plan details before the visit, submitted as an electronic transaction through DHPO.
- Pre-authorization (where required): For services that need prior approval, the clinic submits a request to the payer through DHPO and waits for a coverage decision.
- Claim submission: After treatment, the clinic compiles the claim — diagnosis codes, procedure codes, charges — and transmits it through DHPO to the correct payer.
- Validation: DHPO runs the claim against DHA’s published business and validation rules. Malformed or incomplete claims are bounced back with an error report before they even reach the payer.
- Adjudication and response: The payer reviews the claim and returns an approval, partial approval, or denial — again routed back through DHPO.
- Resubmission (if needed): Denied or flagged claims can be corrected and resubmitted, though resubmission windows and rules apply.
Every one of these steps is a potential failure point, and each one leaves a timestamped record that DHA and payers can review. This is precisely why compliance here isn’t just about “getting claims through” — it’s about getting them through correctly, on time, and in a way that holds up under audit.
DHPO and the ePrescription (eRx) Cycle
Claims aren’t the only thing travelling through DHPO. As eClaimLink expanded to cover the full billing cycle, DHA extended the system to carry electronic prescriptions as well, through what’s commonly referred to as the eRx Hub. When a physician writes a prescription for an insured patient, that prescription transmits electronically through DHPO, and the payer returns real-time coverage feedback before the patient even leaves the consultation room.
This matters for compliance in two ways. First, an eRx reference number is required for insured patients — without one, the payer’s system will automatically reject the related claim, flagged under a denial code tied to the missing reference. Second, cash-paying patients are also folded into the eRx cycle in Dubai, so even non-insurance prescriptions need to be logged through the system correctly. For clinics that dispense medication in-house or run an attached pharmacy, this is effectively a second compliance thread running parallel to claims submission — one that’s easy to overlook if your team’s attention is focused mainly on the billing side of DHPO.
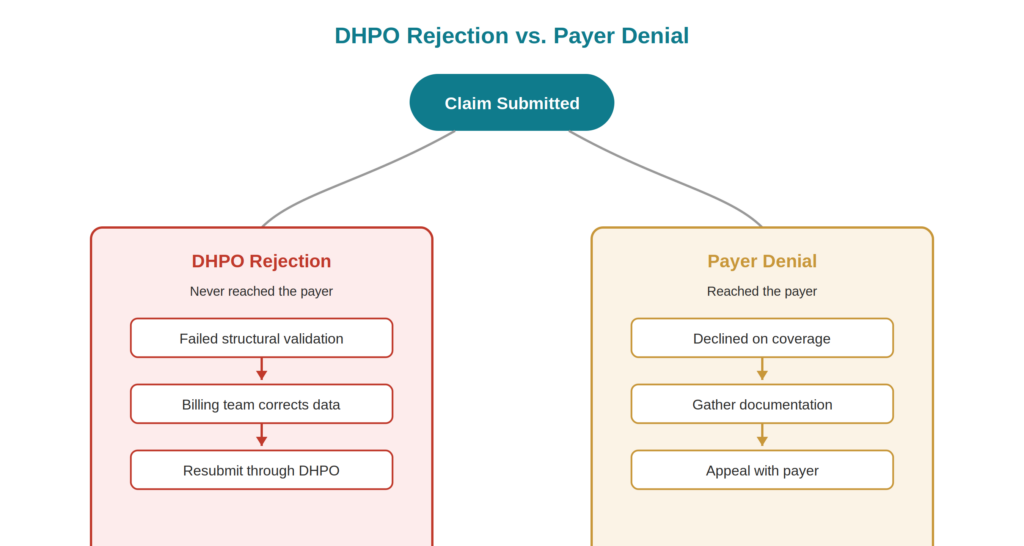
What Happens When a Claim Is Rejected
Rejections at the DHPO level and denials at the payer level are two different things, and clinics sometimes conflate them. A DHPO-level rejection means the claim never made it to the payer at all — it failed DHA’s structural validation rules (a missing field, an invalid code, a formatting error) and bounced straight back to the clinic with an error report. A payer-level denial means the claim reached the insurer and was declined on clinical or coverage grounds — a service not covered under the patient’s plan, or a missing pre-authorization, for example.
The distinction matters because the fix is different in each case. A DHPO rejection is usually a data quality issue your billing team can correct and resubmit quickly, without involving the payer at all. A payer denial often needs supporting clinical documentation, a formal appeal, or direct follow-up with the payer’s claims department. Clinics that track these two categories separately tend to spot patterns faster — realizing, for instance, that one particular procedure code keeps triggering DHPO validation errors, which points to a coding template that needs fixing at the source rather than being corrected claim by claim, every time it comes up.
The Compliance Layer: Timelines Under PD-05-2025
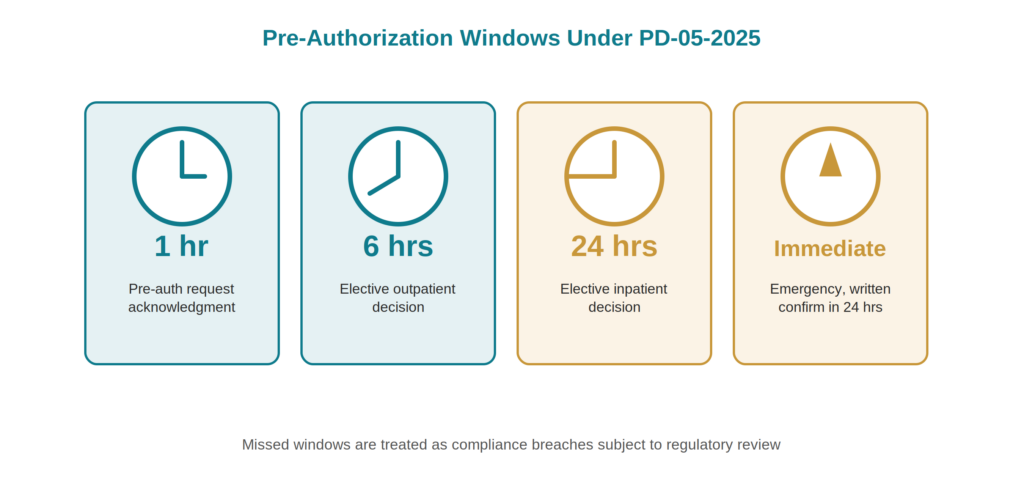
Dubai’s claims management regulation, PD-05-2025, sets specific timing obligations that clinics submitting through DHPO need to build into their workflow. These aren’t suggestions — missed windows are treated as compliance breaches subject to regulatory review.
- Pre-authorization request acknowledgment: Within 1 hour of receipt from the attending physician or clinical department
- Elective outpatient (OP) pre-auth decision: Within 6 hours of the request
- Elective inpatient (INP) pre-auth decision: Within 24 hours of the request
- Emergency authorization: Processed immediately, with written confirmation to follow within 24 hours of verbal approval
If your clinic’s front desk or billing team is manually keying pre-authorization requests into a portal one at a time, hitting these windows consistently is difficult. This is one of the more concrete, practical arguments for EMR-integrated DHPO submission over manual portal use — timing compliance becomes a system function rather than something dependent on staff bandwidth.
Manual Portal Use vs. EMR Integration
| Manual DHPO Portal | EMR-Integrated Submission | |
| Best suited for | Very low claim volumes | Clinics with regular insured patient flow |
| Error risk | Higher — manual re-entry across systems | Lower — data flows directly from patient record |
| Timeline compliance | Dependent on staff availability | Supported by automated submission and alerts |
| Audit trail | Fragmented across separate logins | Centralized within the patient’s clinical and billing record |
| Staff time | Significant, scales poorly with volume | Reduced, scales with clinic growth |
Neither path is inherently non-compliant — DHA doesn’t mandate EMR integration specifically. But as claim volume grows, the operational reality of PD-05-2025’s timelines tends to make manual portal use a diminishing option.
Common DHPO Compliance Pitfalls
Where clinics most often run into trouble:
- Treating DHPO and NABIDH as one obligation. Confirming your DHPO claims integration is live doesn’t tell you anything about your NABIDH clinical data compliance — they’re checked separately during inspections.
- Missing pre-authorization windows. A one-hour acknowledgement window leaves little room for manual bottlenecks, especially during peak clinic hours.
- Inconsistent coding across claims. Validation errors at the DHPO level are often the first sign of a coding or documentation gap that would otherwise surface later as a payer audit finding.
- Assuming eligibility once means eligibility always. Coverage can change between visits; re-verifying through DHPO before each treatment episode avoids denials tied to lapsed or altered policies.
A Practical Compliance Checklist
- Confirm your clinic’s DHPO integration is active and registered under your correct DHA facility license.
- Map your internal claim workflow against the PD-05-2025 timelines and identify where staff-dependent steps could cause delays.
- Review your claim rejection and denial reports monthly to catch recurring validation errors before they compound.
- Keep DHPO and NABIDH compliance as separate tracking items — don’t assume one covers the other.
- If claim volume has grown since your last system review, evaluate whether manual portal submission still fits your clinic’s size.
- Document your pre-authorization and eligibility check processes so timing compliance can be demonstrated during an inspection, not just assumed.
Building DHPO Compliance Into Staff Training
Systems don’t create compliance on their own — the people entering data into them do. A clinic can have a fully integrated, technically sound DHPO connection and still generate a steady stream of rejections if front-desk and billing staff aren’t trained on what the system actually needs from them at each step.
A few practices worth building into onboarding and refresher training for any staff member touching claims:
- Coding consistency: Staff entering diagnosis and procedure codes should understand not just how to select a code, but which ones commonly trigger DHPO validation errors for your clinic’s specialty.
- Eligibility verification habits: Make re-checking eligibility before each visit a standard step, not an exception handled only when something looks unusual.
- Pre-authorization ownership: Assign clear responsibility for who initiates pre-auth requests and who tracks the response window, so a one-hour deadline doesn’t quietly slip because no one owned the follow-up.
- Rejection triage: Train staff to distinguish a DHPO-level rejection from a payer-level denial at a glance, so the right person handles the right problem without delay.
Clinics that revisit this training periodically — rather than only at onboarding — tend to see fewer repeat errors, since DHA and payer validation rules do get updated from time to time, and staff need a reliable way to stay current.
DHPO isn’t a system you configure once and forget. It’s an ongoing operational discipline — one that touches your front desk, your billing team, and ultimately your clinic’s cash flow. Clinics that treat it as a compliance checkbox tend to discover the gaps during an inspection. Clinics that build it into their daily workflow tend to find claims moving faster, with fewer surprises.
Simplify Your DHPO Claims Workflow
Note: Balsam Medico provides clinic management and EMR software with DHPO-integrated claims submission. This article relays regulatory information for awareness — it is not a substitute for DHA’s official circulars or legal advice, and Balsam Medico does not provide licensing or regulatory representation services on a clinic’s behalf.
Balsam Medico’s clinic management system integrates directly with DHPO and eClaimLink, helping your billing team meet submission timelines, reduce rejected claims, and keep a clean audit trail — without the manual portal juggling.
Connect with Us
Ready to embark on this exciting journey? Contact us today:
📍 Dubai, United Arab Emirates – Tel: +971 56 640 9602
📍 Khartoum, Sudan – Tel: +249 91 273 1048
Explore Balsam Medico and discover a world of efficient clinic management at www.balsammedico.com. Together, let’s reduce fines, elevate efficiency, and embrace a new era of dental healthcare.
One last thing..
PS: We built Balsam Medico to be the best software for clinics in UAE and the middle east. It is powerful, flexible, and most importantly, very easy to use.
If you have two minutes, see how it works.
This is the main landing page to learn more.